
Ankylosing spondylitis: natural support for patients
IMPORTANT: Ankylosing spondylitis is a chronic, progressive inflammatory rheumatic disease that requires specialized medical treatment: non-steroidal anti-inflammatory drugs, biologic therapies (anti-TNF, anti-IL17), physiotherapy. There is no natural cure that can heal the disease or stop spinal ankylosis. Everything that follows is strictly intended as an adjunct to the treatment prescribed by a rheumatologist. Any change in diet, supplements, or herbs must be discussed with your doctor.
Ankylosing spondylitis, or AS as patients often call it, is not a disease you control on your own. It is a lifelong journey walked side by side with your rheumatologist and physiotherapist. But once medical treatment is in place, lifestyle weighs enormously. The way you move in the morning, how you sleep, what you eat, whether you smoke, how you manage stress, all of these make the difference between a spine that stays mobile and one that slowly stiffens.
The disease occurs when the immune system attacks the sacroiliac joints and, over time, the vertebrae, ligaments, and even some peripheral joints. New bone forms where it should not, and the spine begins to fuse. If not stopped, the disease leads to a rigid, forward-bent spine known in medicine as a bamboo spine. Fortunately, modern treatments, especially biologic therapies, have dramatically changed the prognosis.
The patient also plays a very active role: daily exercise, correct posture, an anti-inflammatory diet, adequate rest. This article gathers, in plain language, what you can do alongside medical treatment.
Contents
- What ankylosing spondylitis is
- Signs and diagnosis
- Why movement is essential
- Useful daily exercises
- Daytime posture, sleep posture
- The diet that supports treatment
- Body weight and smoking
- Herbs and supplements with possible effect
- Practical tips
- Frequently asked questions
What ankylosing spondylitis is
Ankylosing spondylitis belongs to axial spondyloarthritis, a group of inflammatory rheumatic diseases that mainly affect the spine and the sacroiliac joints. It is not a degenerative disease like osteoarthritis, but an autoimmune one with chronic inflammation. It occurs more often in young men, between 17 and 35 years old, although women can also develop milder forms. There is a strong genetic component: over 85% of patients carry the HLA-B27 gene.
How it presents
- Lower back and buttock pain, especially at night and in the morning
- Morning stiffness lasting more than 30 minutes
- Pain improves with movement, worsens at rest
- Sometimes pain at the sternum, ribs, heel, or other joints
- Chronic fatigue
- In more severe forms, limited spinal flexion and kyphosis
Inflammation can also affect the eyes (uveitis), skin, intestines (associated Crohn disease or ulcerative colitis), sometimes the aortic valve. This is why AS is not just a spinal problem.
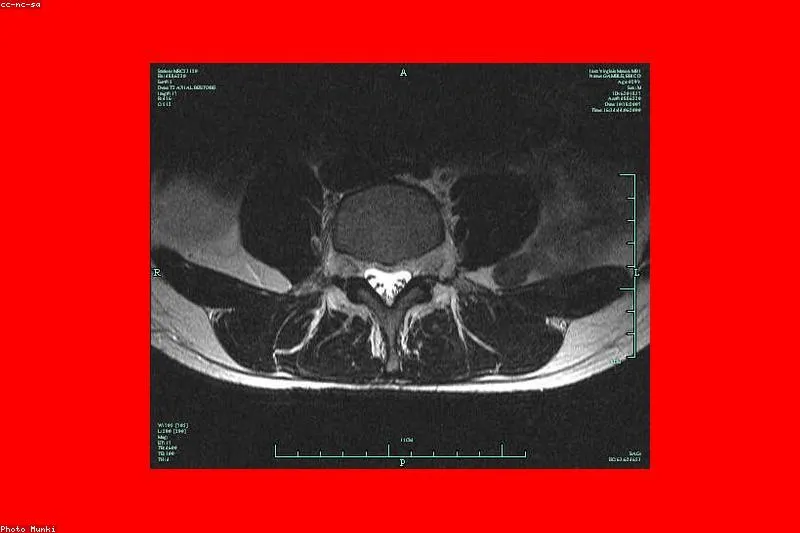
When it is suspected
A young man with low back pain lasting more than three months, waking him at night and improving with movement rather than rest, is a typical case. The rheumatologist will examine the patient clinically, order an MRI of the sacroiliac joints and inflammation markers (ESR, C-reactive protein), and sometimes the HLA-B27 test.
Signs and diagnosis
The diagnosis is made by the rheumatologist based on ASAS criteria: inflammatory back pain lasting more than three months, onset before age 45, plus imaging signs (sacroiliitis on MRI or X-ray) or HLA-B27 positivity plus other clinical criteria. The diagnosis is not guessed, because other conditions can cause similar pain: disc herniation, fibromyalgia, severe osteoarthritis.
A complete workup also includes tendon and peripheral joint ultrasound, tests to rule out other diseases, and ophthalmology evaluation for uveitis if needed. Good documentation from the start is important, because modern treatments, especially biologics, can only be prescribed after strict criteria are met.
Why movement is essential
If you ask any rheumatologist what the non-pharmacological pillar of AS is, the answer will be the same: exercise. Physiotherapy is not optional, it is an integral part of treatment. A patient who exercises daily, even for just 30 minutes, maintains spinal mobility much better, breathes more easily, and feels less pain.
Movement does several things at once: it maintains spinal range, strengthens back muscles, improves breathing (AS can limit chest expansion), reduces stiffness, and improves mood. When you do not move, pain does not calm down, it becomes worse. It seems paradoxical, but that is the nature of the disease.
Recommended types of exercise
- Flexibility exercises for spine, neck, shoulders
- Postural exercises to maintain extension
- Breathing exercises to expand the rib cage
- Strengthening exercises for back and abdominal muscles
- Swimming, one of the best activities, because it unloads joints
- Yoga adapted, with a teacher who knows the disease
What is not recommended: contact sports, heavy lifting with poor technique, activities with high fall risk.
Useful daily exercises
Here is a short routine the patient can do in the morning, after warm shower water has loosened the body. It is only an example; the actual plan must be set by the physiotherapist.
- Lying on the back, stretching the spine with arms above the head, held for 30 seconds
- Pelvic tilts lying on the back with knees bent
- Spinal flexion seated, slowly lowering the trunk between the knees
- Seated trunk rotation with hands on shoulders
- Spinal extension at the edge of the bed, trunk extended slightly over the edge
- Deep diaphragmatic breathing, 10 cycles, with wide inhalation through the nose
- Shoulder rolls, gentle neck rotations, without abrupt movements
If possible, swimming two or three times a week is gold for the AS patient. The warm water of a rehabilitation pool is especially beneficial.
Daytime posture, sleep posture
AS tends to pull the trunk forward. For this reason, everything about posture matters enormously. Sitting at a desk, behind the wheel, in front of the TV, all these prolonged positions, if done with a curved back, accelerate the stiffening of the spine into kyphosis.
A few simple rules
- A chair with good lumbar support
- Monitor at eye level
- Stretch breaks every 45 minutes
- Avoid prolonged sitting on soft sofas
- Bag on the back, not on a single shoulder
For sleep, the recommended position is on the back, with a thin pillow. A firm mattress, not too soft, not too hard. Sleeping on the stomach with the head turned is not ideal, but worse is curled-up sleep, which encourages kyphosis.
A posture check exercise
Stand with your back against a wall: heels, buttocks, shoulders, and head should touch the wall. If your nape does not reach the wall without effort, your posture needs work. Do this test from time to time; it is a useful signal of disease progression.
The diet that supports treatment
There is no diet that cures AS. But there are food choices that reduce background inflammation. Patients who adopt a Mediterranean-style diet often report less pain, more energy, and easier weight control.
What to put on the table
- Fatty fish (salmon, mackerel, sardines, herring) two or three times a week
- Extra virgin olive oil as the main fat
- Fresh seasonal vegetables, as colorful as possible
- Berries, rich in antioxidants
- Legumes: beans, lentils, chickpeas
- Whole grains, in moderation
- Nuts, seeds, avocado
- Herbal teas, still water, coffee in moderation
What is good to limit
- Processed meats (sausages, cold cuts)
- Added sugar, sweetened drinks
- White flour, pastries
- Alcohol in excess
- Trans fats from ultra-processed foods
- Salt above need
Some patients report that when they reduce gluten or dairy, they feel better. There is no solid evidence for all patients, but if you notice a link for yourself, it is worth exploring with a nutritionist. Do not cut out entire food groups without proper replacement.
Body weight and smoking
Two simple things, but huge in impact. Extra kilos press on an already suffering spine and worsen pain. Losing a few kilograms can make the difference between agonizing mornings and reasonable mornings.
Smoking is even worse. In spondylitis patients, smoking accelerates disease progression, reduces the effectiveness of biologic therapies, and worsens respiratory capacity, which can already be limited by rib cage stiffening. Quitting smoking is one of the most powerful tools the patient has.
Herbs and supplements with possible effect
A few options can support inflammation control as an adjunct. None replaces prescribed treatment.
- Turmeric (curcumin): moderate anti-inflammatory effect. Taken with black pepper for absorption. Watch for interactions with anticoagulants.
- Omega 3 from fish oil: helps reduce systemic inflammation. Usual dose 1-2 g EPA+DHA per day.
- Vitamin D: often deficient in autoimmune patients. Blood levels are measured and supplementation is based on results.
- Ginger: as tea or fresh root, mild anti-inflammatory effect.
- Boswellia serrata: extract with some evidence in inflammatory arthritis, to be discussed with the doctor.
- Frankincense (aromatherapy): no proven benefits for AS, but can help with relaxation.
Warm teas, warm baths (not very hot), moderate saunas can temporarily relieve pain without halting the disease. Thermal bath cures at specialized resorts are a useful tradition, especially those with sulfurous or salted waters.
Practical tips
- Start the day with five minutes of in-bed warm-up, then a warm shower.
- Schedule physiotherapy two or three times a week.
- Keep a short pain and activity journal. It helps at rheumatology visits.
- Do not skip medication even on good days.
- Set alarms for movement breaks at work.
- Avoid prolonged cold and dampness, they stiffen joints.
- Take care of your eyes: for any redness, pain, or light sensitivity, go urgently to the ophthalmologist (uveitis suspicion).
- Talk openly with family about what you can and cannot do.
Moments that call for urgent evaluation
Severe chest pain, new vision changes, persistent fever, worsening nocturnal pain not relieved by medication, sudden loss of sensation or strength in limbs. Any of these signs needs urgent medical evaluation.
Medical treatment, the central pillar
Before anything, it is important to come back to prescribed treatment. The first step is non-steroidal anti-inflammatory drugs, used properly under medical supervision, because they can affect stomach and kidneys. In patients with active disease despite NSAIDs, biologic therapy is introduced: anti-TNF (adalimumab, etanercept, infliximab) or anti-IL17 (secukinumab, ixekizumab). These therapies have radically changed the quality of life of AS patients.
When needed, sulfasalazine or methotrexate are also used, especially for peripheral forms. Local injections can help for enthesitis or isolated arthritis. Surgery is rarely used, in severe forms, for kyphosis correction or hip replacement.
All natural advice in this article sits on top of medical treatment, never replaces it. Real effectiveness comes from that combination: modern medication plus movement, plus nutrition, plus quitting smoking, plus psychological support when needed.
Frequently asked questions
Can I live a normal life with ankylosing spondylitis? Yes, in most cases. With early diagnosis, correct treatment, and adherence to the exercise program, many patients work, play sports, have families, travel. There are more severe forms that limit activities, but they are becoming rarer thanks to biologic therapies.
Why does my pain improve with movement and worsen at rest? It is the typical sign of inflammatory pain. Unlike mechanical pain (for example, disc herniation) which improves at rest, in AS inflammation accumulates during inactivity. This is one of the major clues that helps the doctor make the diagnosis.
I am HLA-B27 positive. Will I definitely get spondylitis? No. Not everyone with HLA-B27 develops spondylitis. The risk is higher than in the general population, but triggering factors (infections, stress, sometimes unknown) also matter. HLA-B27 is a risk factor, not a sentence.
Can you have a pregnancy with ankylosing spondylitis? Yes, you can. Pregnancy planning is done together with the rheumatologist, because some medications must be stopped or switched. During pregnancy, the disease behaves variably: some patients feel better, others worse. Post-partum flares can occur, so monitoring is needed.
Are thermal baths useful? Yes, balneotherapy and hydrotherapy are well known adjuncts. Sulfurous, saline, or mesothermal waters are traditionally used. But they do not replace medication. A patient undergoing a spa cure should stay on prescribed treatment and discuss adjustments with the doctor.
How long does morning stiffness last in an AS patient? Typically more than 30 minutes, sometimes one or two hours. With correct treatment and daily exercise, this time decreases significantly. If stiffness returns or lengthens, it is a sign the disease is not well controlled and needs reassessment.
Is ankylosing spondylitis contagious? No. It is not transmitted in any way. It is an autoimmune disease with a genetic component. In families with affected members, the risk is slightly higher, but the disease is not caught through contact.
Conclusion
Ankylosing spondylitis is a diagnosis that frightens at first. The truth is that today, with modern medication and an active movement program, patients live full lives. The secret is the combination between the rheumatologist who leads treatment and the patient who does their part: daily exercises, careful posture, smart nutrition, quitting smoking, attention to body signals. Nature helps, but does not do all the work. Modern medicine helps, but without your daily discipline, results are half as good. Together, it works. Be patient, be consistent, ask for support when you need it. Your spine will thank you.